


CATARACT IN CHILDREN FAQ
FAQ
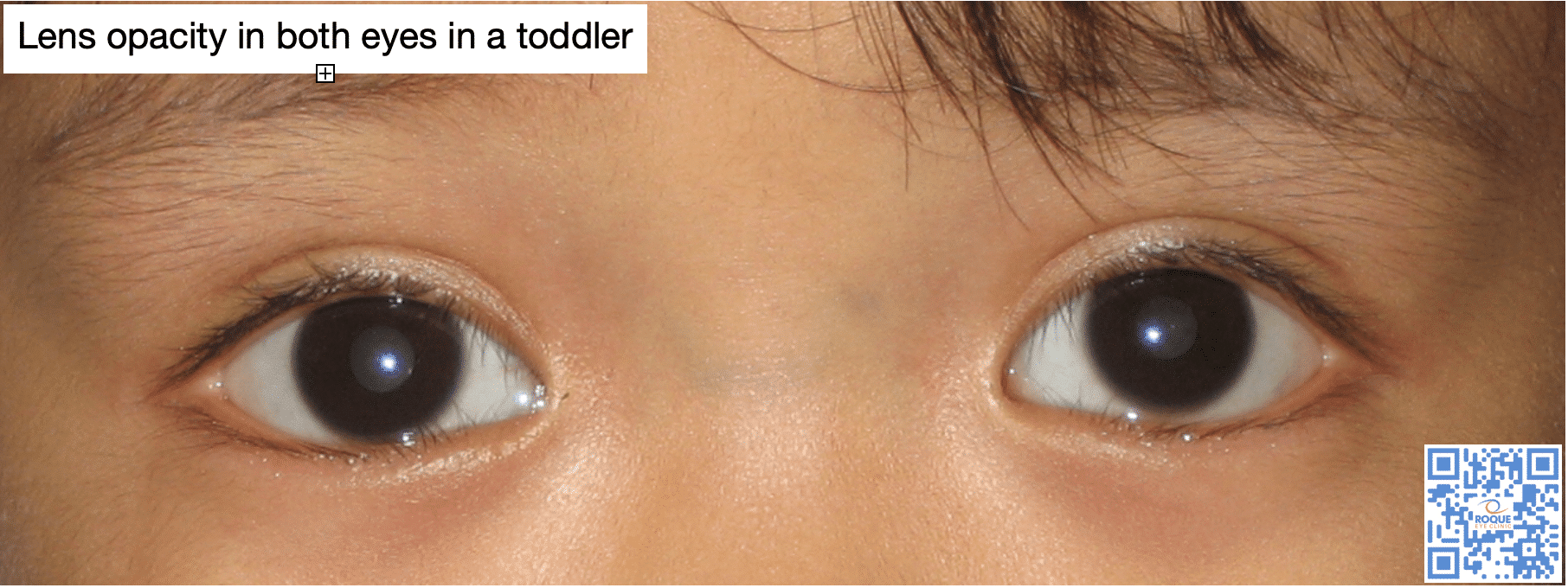
Cataract is the whitening of the natural lens of the eye. It is an aging-related condition seen in adults but it can also occur in children. Cataract in children may be an effect of any of a variety of causes.
It can be hereditary, when it is passed on from one generation to another (autosomal dominant, autosomal recessive, or x-linked recessive). It can be caused by a metabolic condition that prevents the eye from maintaining its clarity (galactosemia, Wilson disease, hypocalcemia, diabetes mellitus). It can come from a developmental insult from an intrauterine infection (TORCHES). It can present as a part of the multiple defects seen in a chromosomal anomaly (Trisomy 21) or a syndrome. It can be associated with other eye abnormalities (posterior lenticonus, lentiglobus, aniridia, anterior segment dysgenesis, persistent hyperplastic primary vitreous, posterior pole tumor). It can be induced by any medication known to cause whitening of the lens, if used for a long time (steroid). It can develop months or years after a blunt or direct trauma to the eye. In majority of cases, however, the cause is unknown (idiopathic).
Although pediatric cataracts have a diverse etiology, with the majority being idiopathic, genetic counseling and molecular testing should be undertaken in hereditary cases.
A comprehensive eye exam in the clinic almost always show the lens opacity, its extent, and if both eyes are involved. However, other diagnostic tests will guide the pediatric ophthalmologist to create a plan of action. A B-scan ultrasound of the eye is important in documenting the status of the internal parts of the eye. A biometry is done to document axial length at the time of diagnosis and is repeated at the time of intraocular lens implantation, and possibly one year after.
Cataract surgery should be done as soon as diagnosed because amblyopia can set in within a few months after birth. The eye undergoes significant development during the first two years of life, therefore, computing for the power of the intraocular lens in infancy is challenging. It is for this reason that IOL implantation as a secondary procedure is a more practical approach. This can be done at age 2, when the eyeball has reached a length that simulates adult average values. Contraindications to IOL implantation include microphthalmos (short eyeball), anterior segment dysgenesis, anatomic problems in the posterior pole, and Congenital Rubella Syndrome (associated with severe inflammation).
There is a higher risk for amblyopia in unilateral cataract. After cataract surgery, the pediatric ophthalmologist will prescribe either aphakic glasses or aphakic contact lenses, while awaiting for the secondary IOL implantation. Amblyopia treatment in the form of patching or atropine eyedrops will be started right after the cataract surgery. Once the proper intraocular lens is implanted, any residual refractive error shall be addressed with glasses. Refraction and measurement of intraocular pressure (to rule out secondary glaucoma) will be done regularly, either in the clinic or in the operating room (under general anesthesia). Post-surgical cataract patients need at least a yearly check until they reach adulthood.
- Bothun, E., Wilson, M., Traboulsi, E., Diehl, N., Plager, D., Vanderveen, D., Freedman, S., Yen, K., Well, N., Loh, A., Morrison, D., Anderson, J., Lambert, S., Toddler Aphakia and Pseudophakia Study Group (2019). Outcomes of unilateral cataracts in infants and toddlers 7 to 24 months of age: Toddler Aphakia and Pseudophakia Study (TAPS). Ophthalmology, 126(8): 1189-1195.
- Chang, P., Lin, L., Li, Z., Wang, L., Huang, J., and Zhao, Y. (2020). Accuracy of 8 intraocular lens power calculation formulas in pediatric cataract patients. Graefes Arch Clin Exp Ophthalmol, epub
- Medsinge, A., and Nischal, K (2015). Pediatric cataract: challenges and future directions. Clin Ophthamol, 7(9): 77-90.

BOOK AN APPOINTMENT
It takes less than 5 minutes to complete your online booking. Alternatively, you may call our BGC Clinic, or our Alabang Clinic for assistance.
OUR DOCTORS

DR. BARBARA ROQUE
MD, DPBO, FPAO, FPCS
Dr. Barbara Roque is a specialist in pediatric ophthalmology, adult strabismus, and ophthalmic genetics. Her private practice began in 2006, after her post-graduate fellowship training at The Children’s Hospital in Westmead, University of Sydney System, Australia. Her patients are mostly children with ocular disease, refractive errors, cataracts, and eye misalignment.

DR. MANOLETTE ROQUE
MD, MBA, DPBO, FPAO, FPCS
Dr. Manolette Roque is a specialist in uveitis, cataract, and refractive surgery. His private practice began in 2000, after his post-graduate fellowship at the Massachusetts Eye and Ear Infirmary, Harvard Medical School, in Boston, Massachusetts, USA. His patients are mostly adults who desire spectacle independence. His advocacy includes taking care of individuals with ocular inflammatory diseases.
Everyone deserves the best eye care possible.
OUR CLINICS
BGC CLINIC
- ST. LUKE'S MEDICAL CENTER GLOBAL CITY
2/F Medical Arts Building 217
Rizal Drive corner 5th Avenue
Bonifacio Global City, Taguig 1634
Philippines
SLMC CLINIC HOURS
- 9am - 12pm
Appointments only
ALABANG CLINIC
- ASIAN HOSPITAL AND MEDICAL CENTER
5/F Medical Office Building 509
2205 Civic Drive, Filinvest City
Alabang, Muntinlupa 1781
Philippines
AHMC CLINIC HOURS
- 1pm - 4pm
Appointments only
BOOK AN APPOINTMENT
It takes less than 5 minutes to complete your online booking. Alternatively, you may call our BGC Clinic, or our Alabang Clinic for assistance.


{kind=link}
{kind=link}
{kind=link}