

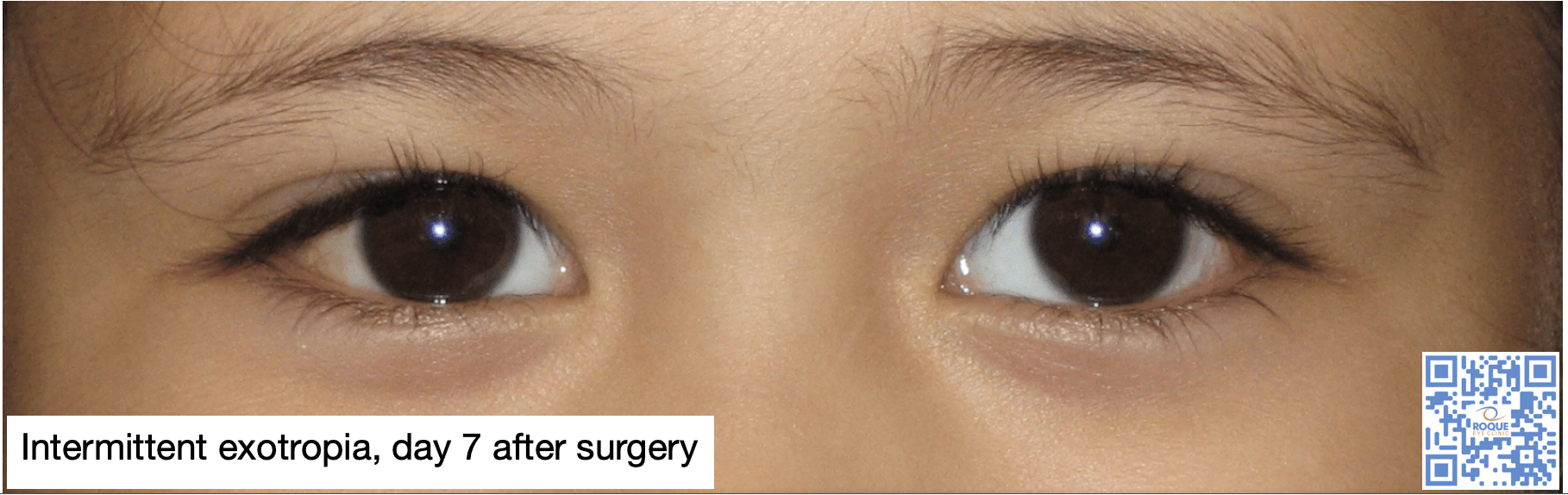
Intermittent Exotropia
Intermittent exotropia is an outward eye deviation that develops shortly after birth. It usually begins as an exophoria, which means that the child’s ability to fuse controls the deviation. This is why some parents deny seeing a deviation when the child was younger. The exophoria may deteriorate over time into intermittent exotropia then constant exotropia, as the brain learns to suppress the image from the deviated eye. Suppression is the reason why affected children do not complain of seeing double. Its presence, however, lowers the success rate of surgery.
Not all cases are progressive so watchful waiting may be a reasonable approach in 12-36 months old but monitoring control, suppression and strereopsis are clinical guides as to the need for surgical intervention.
Part-time alternate occlusion and overminus spectacles (for myopes) is significantly effective on control of small angle intermittent exotropia. It is a useful method to postpone or even eliminate the need for surgery in this subset of patients.
The goal of surgery in intermittent exotropia is to preserve binocularity and stereopsis (depth perception). Surgery should be contemplated when: (1) the angle of deviation is increasing, (2) there is deterioration in control (increase in frequency of manifest exotropia), (3) there is decrease in stereopsis (depth-perception) for distance and near, and (4) there is an effect on the quality of life of the patient.
Bilateral lateral rectus muscle recession and unilateral lateral rectus recession with medial rectus resection, are the two most common surgical procedures performed for intermittent exotropia. However, exotropic drift is more commonly seen in unilateral recess-resect procedure compared to the symmetric bilateral lateral recession technique.
Children who are operated on at a younger age, between 3-5 years old, have better surgical outcomes. Overcorrection (small esotropia after surgery) rather than orthotropia should be the target immediate postoperative deviation angle, to offset the exotropic drift. Recovery from suppression is not a guarantee after surgery when the angle of deviation is large.
- Chougule, P., and Kekunnaya, R. (2019). Surgical management of intermittent exotropia: do we have an answer for all? BMJ Open Ophthalmol, 4(1): e.000243.
- Cotter, S., Mohney, B., Chandler, D., Holmes, J., Wallace, D., Melia, B., Wu, R., Kraker, R., Superstein, R., Crouch, E., Paysse, E.; Pediatric Eye Disease Investigator Group (2020). Three-year observation of children 12 to 35 months old with untreated intermittent exotropia. Ophthalmic Physiol Opt, 40(2): 202-215.
- Huh, J., Ha, S., and Kim, S. (2020). Recovery from suppression with successful motor alignment after surgery for intermittent exotropia. J Pediatr OIphthalmol Strabismus, 57(1): 51-56.
- Kushner, B. (2019). Conservative management of intermittent exotropia to defer or avoid surgery. J AAPOS, 23(5): 256.e1-256.e6.
- Repka, M., Chandler, D., Holmes, J., Donahue, S., Hoover, D., Mohney, B., Philips, P., Stout, A., Ticho, B., Wallace, D.; Pediatric Eye Disease Investigator Group. (2020). The relationship of age and other baseline factors to outcome of initial surgery for intermittent exotropia. Am J Ophthalmol, 212: 153-161.
- Sung, J., Yang, H., and Hwang, J. (2020). Comparison of surgery versus observation for small angle intermittent exotropia. Sci Rep, 10(1): 4631.
- Xie, F., Zhao, K., and Zhang, W. (2019). Comparison of surgical outcomes between bilateral lateral rectus recession and unilateral recession-resection in moderate angle intermittent exotropia. J AAPOS, 23(2): 79.e1-79.e7.
- Yoo, G., Ha, S., and Kim, S. (2019). Distance suppression as a predictive factor in progression of intermittent exotropia. Korean J Ophthalmol, 33(5): 446-450.


{kind=link}
{kind=link}
{kind=link}